
Diagnostic Considerations For The Edentulous Maxilla
What are some of the diagnostic considerations prior to treatment with a fixed maxillary implant supported prosthesis? In this issue, we will address some of the most important factors we need to consider.
Maxillary incisal edge position: This is generally determined by evaluation of the esthetics and phonetics of an existing maxillary denture or new denture being fabricated.
Phonetics: Maxillary teeth should be positioned such that the incisal edges gently touch the wet–dry junction of the lower lip upon enunciation of “F” and “V” sounds.
Esthetics: An assessment of the display of maxillary central incisors when lips are in repose should be made. This will help render an esthetic tooth set up.
The combination of the phonetics and esthetics assessment will ultimately determine the appropriate incisal edge position.
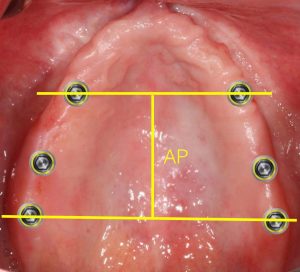
Arch form: The maxillary arch form provides the osseous foundation for the implants, tooth position, and the implant “A-P spread”. Generally, maxillary arch forms are ovoid (58%), square (32%), and tapered (10%). The AP (Antero-posterior) spread denotes a distance measurement from the center of the two most anterior implants to the distal aspect of the two most posterior implants. The AP spread can be multiplied by 1.5 for a guideline of how long of a distal cantilever might be acceptable. The measurement is only a guideline. This is not a set rule and many factors need to be considered. The following illustrations demonstrate proposed A-P spreads and implant distribution for different arch forms.

Ovoid

Square
Tapering
Maxillomandibular relationship: The superior and medial pattern of resorption of the maxillary arch post extraction could alter the arch form. In the anterior maxilla, horizontal bone resorption is twice as pronounced as vertical resorption. However, horizontal and vertical atrophy in the posterior maxilla occurs at the same rate. These varying patterns of resorption could render maxillo-mandibular jaw relationships that are different from the patient’s natural jaw relationship prior to extraction and healing.
 Maxillary lip position and ridge display: 70% of the general population exhibits an “average smile”, displaying 75 to 100% of maxillary incisors and interproximal gingiva. Individuals with a “high smile” display 100% of maxillary anterior tooth length as well as a contiguous band of gingiva. “Low smile” displays less than 75% of maxillary anterior tooth length. From a maxillary fixed prosthetic restoration standpoint, “high smile” patients are the most challenging to treat. When edentulous, these patients often carry-over their condition, displaying their residual alveolar ridge upon maximum animation, leading to the visibility of the prosthetic-tissue junction and an unacceptable esthetic result.
Maxillary lip position and ridge display: 70% of the general population exhibits an “average smile”, displaying 75 to 100% of maxillary incisors and interproximal gingiva. Individuals with a “high smile” display 100% of maxillary anterior tooth length as well as a contiguous band of gingiva. “Low smile” displays less than 75% of maxillary anterior tooth length. From a maxillary fixed prosthetic restoration standpoint, “high smile” patients are the most challenging to treat. When edentulous, these patients often carry-over their condition, displaying their residual alveolar ridge upon maximum animation, leading to the visibility of the prosthetic-tissue junction and an unacceptable esthetic result.
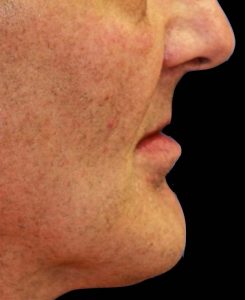
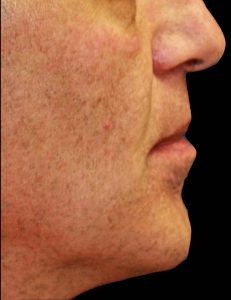 Lip support: lip support is very difficult to quantify. Patient input is paramount to the final determination of an acceptable lip projection. Lip support is dependent upon many factors to include the nasolabial angle and alveolar bone resorption. The nasolabial angle (NLA) for men is averaged to be between 90 to 95 degrees; the average NLA for women is between 95 to 105 degrees. Severity of the alveolar ridge resorption and resulting maxillomandibular ridge relationship might dictate the need for a flanged prosthesis replacing the lost hard and soft tissues. If a flanged prosthesis is indicated, that would exclude the option for a fixed prosthesis due to the inability for adequate at home oral hygiene. One simple method of determining the need for a flanged vs non-flanged prosthesis is to have the patient try out a flanged and a non-flanged mock up. If the nasiolabial angle of the patient greatly exceeds 90 degrees while wearing a non- flanged prosthesis, indicating insufficient lip support, then a flanged removable prosthesis may be indicated. If the nasolabial angle is unchanged with a non-flanged prosthesis, then a fixed prosthesis could be considered as the maxillary bone resorption is minimal. It is important to remember that lip support is mostly influenced by the incisal 1/3 of the anterior teeth.
Lip support: lip support is very difficult to quantify. Patient input is paramount to the final determination of an acceptable lip projection. Lip support is dependent upon many factors to include the nasolabial angle and alveolar bone resorption. The nasolabial angle (NLA) for men is averaged to be between 90 to 95 degrees; the average NLA for women is between 95 to 105 degrees. Severity of the alveolar ridge resorption and resulting maxillomandibular ridge relationship might dictate the need for a flanged prosthesis replacing the lost hard and soft tissues. If a flanged prosthesis is indicated, that would exclude the option for a fixed prosthesis due to the inability for adequate at home oral hygiene. One simple method of determining the need for a flanged vs non-flanged prosthesis is to have the patient try out a flanged and a non-flanged mock up. If the nasiolabial angle of the patient greatly exceeds 90 degrees while wearing a non- flanged prosthesis, indicating insufficient lip support, then a flanged removable prosthesis may be indicated. If the nasolabial angle is unchanged with a non-flanged prosthesis, then a fixed prosthesis could be considered as the maxillary bone resorption is minimal. It is important to remember that lip support is mostly influenced by the incisal 1/3 of the anterior teeth.
If you have a question about a case and want another opinion, give us a call.
Comments closed
No comments. Leave first!